A non-invasive Vascular exam is used to assess the circulation and heeling potential of extremities. The Ankle Brachial Index (ABI) is the most common non-invasive vascular exam, it is calculated as ratio of the blood pressure in the lower legs to the blood pressure in the arms. Compared to the arm, lower blood pressure in the leg is an indication of blocked arteries (peripheral vascular disease or PVD). The ABI is calculated by dividing the systolic blood pressure at the ankle by the systolic blood pressures in the arm.[1]
Non-invasive Vascular Exam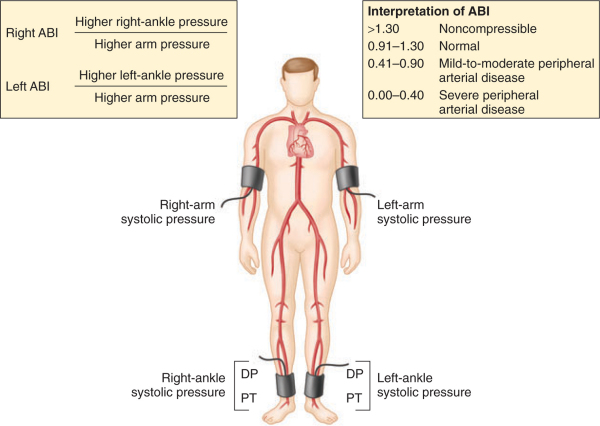
Method
A Doppler ultrasound blood flow detector, commonly called Doppler Wand or Doppler probe, and a sphygmomanometer (blood pressure cuff) are usually needed. The blood pressure cuff is inflated proximal to the artery in question. Measured by the Doppler wand, the inflation continues until the pulse in the artery ceases. The blood pressure cuff is then slowly deflated. When the artery’s pulse is re-detected through the Doppler probe the pressure in the cuff at that moment indicates the systolic pressure of that artery.
The higher systolic reading of the left and right arm brachial artery is generally used in the assessment. The pressures in each foot’s posterior tibial artery and dorsalis pedis artery are measured with the higher of the two values used as the ABI for that leg.[2]
- Where PLeg is the systolic blood pressure of dorsalis pedis or posterior tibial arteries
- and PArm is the highest of the left and right arm brachial systolic blood pressure
The ABPI test is a popular tool for the non-invasive assessment of PVD. Studies have shown the sensitivity of ABPI is 90% with a corresponding 98% specificity for detecting hemodynamically significant (Serious) stenosis >50% in major leg arteries, defined by angiogram.[3]
However, ABPI has known issues:
- ABPI is known to be unreliable on patients with arterial calcification (hardening of the arteries) which results in less or incompressible arteries,[4] as the stiff arteries produce falsely elevated ankle pressure, giving false negatives[5]). This is often found in patients with diabetes mellitus[6](41% of patients with peripheral arterial disease (PAD) have diabetes[7]), renal failure or heavy smokers. ABPI values < 0.9 & >1.3 should be investigated further regardless.
- Resting ABPI is insensitive to mild PAD.[8] Treadmill tests (6 minute) are sometimes used to increase ABPI sensitivity,[9] but this is unsuitable for patients who are obese or have co-morbidities such as Aortic aneurysm, and increases assessment duration.
- Lack of protocol standardisation,[10] which reduces intra-observer reliability.[11]
- Skilled operators are required for consistent, accurate results.[12]
When performed in an accredited lab, the ABI is a fast, accurate, and painless exam, however these issues have rendered ABI unpopular in primary care offices and symptomatic patients are often referred to specialty clinics[13] due to the perceived difficulties. Technology is emerging that allows for the oscillometric calculation of ABI, in which simultaneous readings of blood pressure at the levels of the ankle and upper arm are taken using specially calibrated oscillometric machines.
Interpretation of results
In a normal subject the pressure at the ankle is slightly higher than at the elbow (there is reflection of the pulse pressure from the vascular bed of the feet, whereas at the elbow the artery continues on some distance to the wrist).
The ABPI is the ratio of the highest ankle to brachial artery pressure. An ABPI between 0.9 and 1.2 considered normal (free from significant PAD), while a lesser than 0.9 indicates arterial disease. An ABPI value greater than 1.3 is also considered abnormal, and suggests calcification of the walls of the arteries and incompressible vessels, reflecting severe peripheral vascular disease.
Provided that there are no other significant conditions affecting the arteries of the leg, the following ABPI ratios can be used to predict the severity of PAD as well as assess the nature and best management of various types of leg ulcers:[2]
| ABPI value | Interpretation | Action | Nature of ulcers, if present |
|---|---|---|---|
| above 1.2 | Abnormal Vessel hardening from PVD |
Refer routinely | Venous ulcer use full compression bandaging |
| 1.0 – 1.2 | Normal range | None | |
| 0.9 – 1.0 | Acceptable | ||
| 0.8 – 0.9 | Some arterial disease | Manage risk factors | |
| 0.5 – 0.8 | Moderate arterial disease | Routine specialist referral | Mixed ulcers use reduced compression bandaging |
| under 0.5 | Severe arterial disease | Urgent specialist referral | Arterial ulcers no compression bandaging used |
Top Rated Products